

Arthrocentesis & Injections: Wrist (Radiocarpal)
Last updated: October 15, 2014
Patient Position: The patient may be seated or lying supine.
Limb Position: The wrist, hand, and forearm should be comfortable and parallel to the ground. A small towel can be rolled into a 3-4 cm elevation and put under the wrist, leaving the wrist slightly downward flexed (10 degrees).
Bony Landmarks: Medially, palpate the tip of the ulnar styloid; laterally, the tip of the radial styloid; and dorsally, the extensor pollicis longus tendon. Draw a line (visually) from the tip of the ulnar to radial styloid (Fig. 3). Ask the patient to fully extend the thumb and note where the extensor pollicis longus tendon rises to bisect this line. The injection site is to the ulnar side of this intersection. Confirm this site by palpating (with a thumb nail) along the radius, moving distally until the depression of the radiocarpal joint is felt.
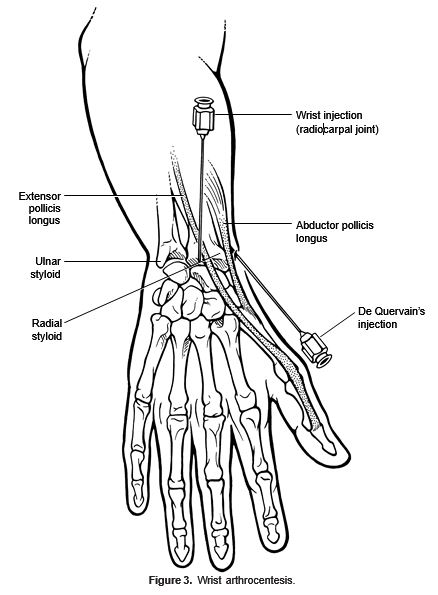
Site/Entry Angle: Using a dorsal (extensor) approach, enter downward at a 90-degree angle to the ulnar side of the extensor pollicis longus tendon (away from the anatomic “snuff box”). The needle should be advanced more than 2 cm into the joint space. Aspirate before injecting.
Amount of Injection: Use a small gauge needle for injection (25-27 gauge) or aspiration (21 gauge) and instill 10 to 40 mg Depo-Medrol (or equivalent), with or without 0.25 mL of 1% lidocaine, in a total volume of 0.5 to 2 mL.
Other Injectable Sites: DeQuervain tenosynovitis, affecting the extensor pollicis brevis and abductor pollicis longus tendons, may be injected with the same amount of steroid preparation. Rotate the hand 90 degrees (thumb up) and place the wrist in slight ulnar deviation. Locate the point of maximal tenderness over the affected tendon. Enter tangentially at a 30-degree angle. Do not inject into the tendon, but close to the tendon sheath.